Bariatric Surgery
Bariatric surgery results in a dramatic change in the patient's stomach anatomy. Due to the reduced food consumption, the body's nutrient and vitamin absorption is impaired, which can lead to severe deficiencies in minerals like iron, vitamin B12, vitamin B1, calcium, zinc, vitamin D and folate.
Visit the Nutrition page for a more detailed breakdown of the minerals you may be deficient in after weight loss surgery, and how LIFE2.0 can help to supplement your diet for a healthier life.
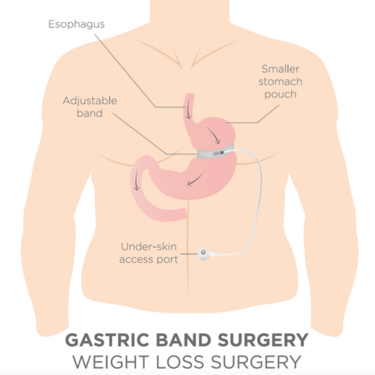
Gastric Band
The gastric band was very popular in the 1990s, and seemed a simple but safe procedure to surgically overcome obesity. Unfortunately, more and more complications emerged as time went on so the original enthusiasm for it faded away. Slippage and erosion are the two most common; these conditions require emergency operations. In addition to this, many patients did not tolerate the restrictions caused by the gastric band, which led to the regaining of weight and a quality of life decrease for some. Because of this, the procedure is now uncommon.
Nevertheless, if you have a gastric band fitted and have no associated health complications, there is no need to have it removed.

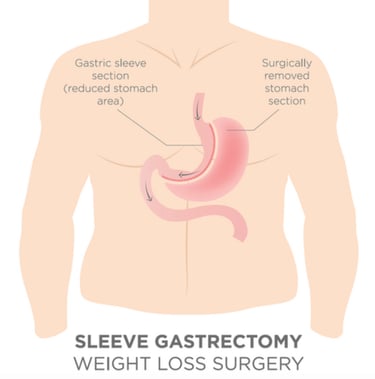
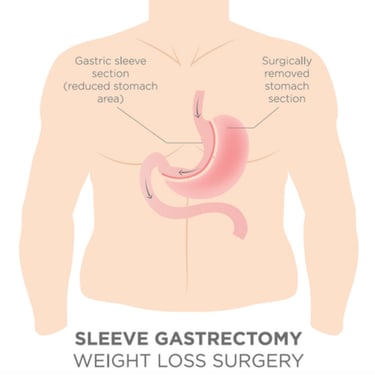
Sleeve Gastrectomy
Recently there has been a significant increase in interest in the sleeve gastrectomy procedure, as it is less complicated than the gastric bypass (mentioned below).
In a sleeve gastrectomy, the volume of the stomach is reduced by 80-85%, and this is physically removed from the body. The consequence of this is that the person can eat much less than before, leading to subsequent weight loss. You are expected to lose around 60% of your pre-existing excess weight, however personal results vary from this statistical average.
Gastric Bypass
Roux-en-Y gastric bypass (RYGB) - more commonly known simply as “gastric bypass” - has long been considered the “gold standard” of bariatric surgery. The operative procedure involves staple-dividing the stomach into two chambers. The upper chamber - called the pouch - receives food and is very small, holding about 20-30 cc. The lower chamber - called the gastric remnant - is “bypassed” and does not receive food. The small intestine is divided at a certain point and one end is connected (“anastomosed”) to the pouch. A second connection (“anastomosis”) is made to connect the disconnected stomach and duodenum to the small bowel. This connection enables the digestive fluids to meet the ingested food to enable nutrient breakdown and absorption. The distance between the two connections can vary by surgeon preference but is generally 50 to 150 cm.
Following bypass surgery, patients can expect to lose around one third of their total body weight, or 70-75% of the original excess weight. The usual weight loss rate is 6 kg (1 stone) per month.

LIFE2.0 Biotechnology Ltd
info@life20vitamins.com
Subscribe to our newsletter
+36 30 2285524

UK customer service number:
+44 20 3129 5383
Terms and conditions